When you hear the word Generic medicines, you might instantly think of words like cheap, ineffective, or maybe even Jan Aushadhi. But the truth is, every branded medicine you take is also a generic medicine. The only difference is that it is marketed under a brand name which makes it expensive. In fact, there is a good chance that your generic medicine and the so-called branded one are made in the same company, just packaged and priced differently.
There are still many myths people hold about generic medicines and that is exactly why this blog is a must read. You have probably been caught in the web of marketing tricks, unknowingly paying for doctor commissions and advertising costs at a heavy price. Read this blog to free yourself from these traps and discover how you can achieve better health and bigger savings without spending more.
Common Myths About Generic Medicines in India Countered with Facts
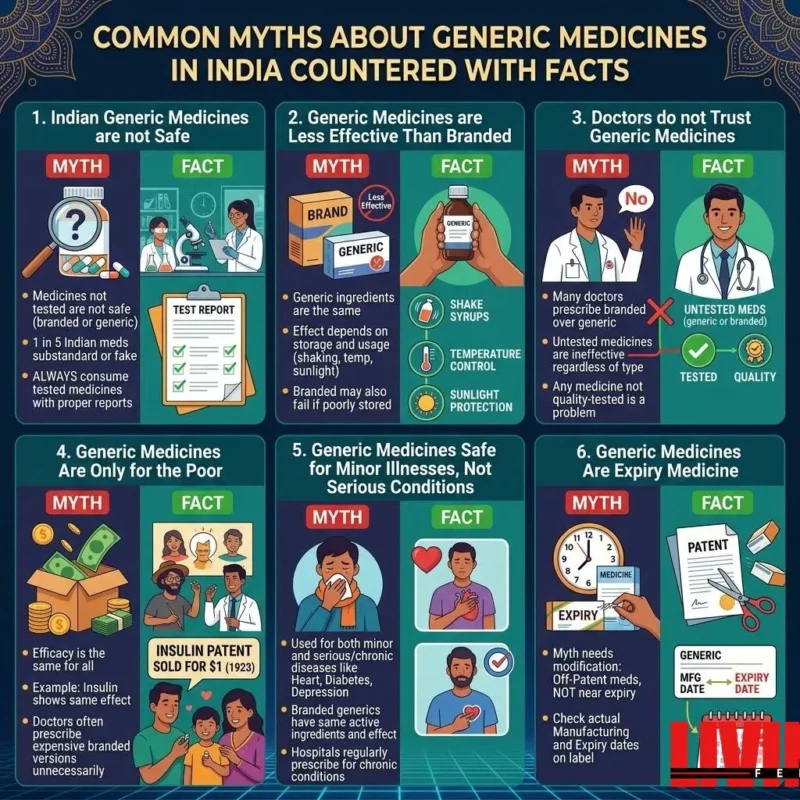
Myth 1: Indian Generic Medicines are not Safe
Fact: People hear “generic” and assume corner-cutting. Cheap packaging, unfamiliar brand name, lower price — must be low quality, right? The fear is understandable, especially when media reports regularly surface about substandard drugs making it into the supply chain.
Medicines, whether branded or generic, in India go through the same regulatory sequence for approval. In India, the Central Drugs Standard Control Organisation (CDSCO) — analogous to the US FDA — mandates that any generic medicine must have the same active ingredient, strength and dosage of a branded version. And the manufacturer also has to show bioequivalence — that the generic sends into your bloodstream at least as much of the drug and within as short a period of time, as the original.
Still, to be fair, the safety concern isn’t totally unfounded — it just focuses on the wrong thing. The actual issues are not generic vs branded. The real disease is untested vs tested. According to a 2017 report from the WHO, it is estimated that approximately 10.5% of medicines in low- and middle-income countries are substandard or falsified (“Substandard and Falsified Medical Products” — WHO, 2017). Similarly, government-sponsored surveys in India over 15 years estimated that around 3% of the market fell within the counterfeit or subpar category although a report put out by Associated Chambers of Commerce and Industry, quoted a much higher estimate (25%) in 2015 (“Impact of Counterfeit Products on Indian Economy” — ASSOCHAM India, 2015)). That difference on its own tells you that this data is disputed, but the take-home message is the same: poor quality medicines exist in both branded and generic forms.
A 2020 study in the Indian Journal of Pharmacology compared branded and branded-generic versions of five widely used medicines — alprazolam, cetirizine, ciprofloxacin, fluoxetine and lansoprazole — made by the same company. Both the brand and generic versions passed all applicable quality tests as per specifications detailed in Indian Pharmacopoeia 2007, including identification, chemical composition, uniformity of content, dissolution studies (“A comparative evaluation of price and quality of some branded versus branded–genetic medicines of same manufacturer in India” — Singal GL et al., Indian Journal of Pharmacology 2011).
Generalise the solution, not avoid generics. It is to take medicines — branded or generic — that have been well tested and carry verifiable quality certification.
Myth 2: Generic Medicines are Less Effective Than the Branded Medicine
Fact: Chemically, the active pharmaceutical ingredient in branded and generic medicines is identical. Which is not an opinion — it’s a regulatory requirement. The US FDA also and CDSCO in India requires bioequivalence of generics with their branded drug counterparts prior to marketing approval. As the US FDA states clearly on their Generic Drugs page, this means that any generic medicine must have the same effect in the body as the brand-name medicine (“Generic Drugs: Questions & Answers” — US FDA).
A 2015 paper in the Journal of Clinical Psychiatry explained how this bioequivalence actually works. A common myth about generics is that they may have anywhere from 80% to 125% of the active ingredient, but this isn’t correct. The bioequivalence is determined by randomised crossover trials comparing two pharmacokinetics parameters — the peak concentration of drug in plasma and area under the curve — between the generic and branded version. This ratio must have a 90% confidence interval between 0.80 and 1.25 for approval (Bioequivalence of generic drugs: a simple explanation for a US Food and Drug Administration requirement Andrade C, Journal of Clinical Psychiatry, 2015).
Where efficacy can actually differ is in storage conditions. Temperature control, sunlight exposure, humidity — all these factors affect a medicine’s stability regardless of whether it is branded or generic. A generic medicine that is improperly stored will lose potency just as fast so an incorrectly stored branded medicine will also. Shaking liquid formulations before use, avoiding moisture for tablets, storing insulin in a refrigerator — these are not optional.
The price difference between branded and generic exists because manufacturers of generics don’t pay for the original drug discovery, clinical trials or the massive marketing budgets that spenders of branded set aside. That difference in cost is a function of business economics, not quality of care.
Myth 3: Doctors do not Trust Generic Medicines
Fact: Not every doctor stays away from generics, but many do in India — and the reasons have more to do with commerce than clinical practice. Covered in proprietary data, pharmaceutical companies spend significantly on marketers to promote their patented products to physicians through medical representatives, conferences, incentives, etc. Recognising that the confidence in generic prescribing should be established for the medical fraternity through better awareness regarding bioequivalence and regulatory standards, a paper published in Journal of Postgraduate Medicine stated so (“Generic drugs – The Indian scenario” — Shetty YC et al., Journal of Postgraduate Medicine, 2019).
Notably, this myth is contradicted by the Indian government own stance. In 2016, the National Medical Commission (formerly known as the Medical Council of India) advised physicians to prescribe medicines in their generic form, which on average cost between 30% and 80% less than their branded counterparts. Government hospitals already run almost exclusively on generic medicines. Public sector doctors surveyed in a BMC Health Services Research study reported giving 99 per cent of medicines as generics, as only government facilities stock generics (“Improving access to medicines by popularising generics: a study of India’s People’s Medicine scheme in two districts of Maharashtra” — BMC Health Services Research (2022).
That study also noted something interesting. Generics did really well for chronic conditions such as diabetes and hypertension, clinicians said. There were some concerns about specific antibiotics, but the issue at hand was over specific manufacturers, not generic medicine itself. Any medicine — brand or generic — made by a manufacturer skimping on quality will be inferior.
Myth 4: Generic Medicines Are Only for the Poor People
Fact: Most of the time it is simply that your doctor is prescribing the expensive branded version of a generic medicine and you end up overpaying without even realizing it.
Consider insulin. In January 1923, Frederick Banting, Charles Best, and James Collip were awarded the American patent for insulin. They sold it to the University of Toronto for $1 each. Their reasoning was straightforward — a life-saving discovery should not be restricted by profit (“The discovery of insulin revisited: lessons for the modern era” — Hirsch IB et al., Journal of Clinical Investigation, 2021). The Snopes fact-check on this event confirms the patent sale happened exactly as described, finalised on January 23, 1923 (“Scientist Sold Insulin Patent for $1, Saying ‘It Belongs to the World’?” — Snopes, 2024).
Actor Fawad Khan, diagnosed with Type 1 diabetes at age 17, has spoken publicly about being on insulin for over 24 years. In an interview with FreeStyle Middle East in 2023, he described how insulin has been part of his daily life since his teenage years (ARY News, 2023). Whether the insulin he uses is a branded formulation or a generic one, the active molecule is the same. The effect it has on his body is the same.
This is true across the board. When a doctor prescribes metformin for diabetes, the branded version and the generic version both contain metformin. A study published in the Journal of Diabetes & Metabolic Disorders found no statistically significant difference in glycated haemoglobin (HbA1c) levels between patients on branded anti-diabetic drugs and those switched to generic alternatives from Jan Aushadhi stores (“Health economics and effectiveness analysis of generic anti-diabetic medication from Jan Aushadhi: An ambispective study in community pharmacy” — Journal of Diabetes & Metabolic Disorders, 2021).
The idea that generics are “for the poor” is not a medical argument. It’s a marketing narrative maintained by companies that benefit from patients choosing the more expensive option.
Myth 5: Generic Medicines is Safe for Minor Illnesses, Not Serious Conditions
Fact: Generic medicines treat the full spectrum of conditions, including the most life-threatening ones. Hospitals across India — government and private — routinely prescribe generic medicines for chronic and severe diseases. The Jan Aushadhi scheme, launched by the Government of India in 2008 and rebranded as the Pradhan Mantri Bhartiya Janaushadhi Pariyojana (PMBJP), stocks medicines for cardiovascular disease, diabetes, mental health disorders, infections, and more — all in generic form (“Why the Jan Aushadhi Scheme Has Lost Its Steam in India?” — Rajagopal D, Journal of Pharmacology and Pharmacotherapeutics, 2017).
A cost analysis published in the Annals of Tropical Medicine and Public Health showed that the branded version of atorvastatin — one of the most commonly prescribed cholesterol-lowering drugs for heart disease — can be 2 to 25 times more expensive than the Jan Aushadhi version. The active ingredient is identical (“A Cost Analysis of the Jan Aushadhi Scheme in India” — Annals of Tropical Medicine and Public Health, 2017).
A Frontiers in Public Health study examining chronic disease medicines found that Jan Aushadhi formulations of Metformin, Amlodipine, and Human Insulin were consistently among the most affordable options available, with branded alternatives carrying cost ratios as high as 7.0 for Metformin (“Medicine affordability and access in India: lessons from generic–branded price variation under the Jan Aushadhi Scheme” — Frontiers in Public Health, 2025).
The only difference between a branded atorvastatin at ₹200 and a generic atorvastatin at ₹15 lies in the price tag. The molecule is the same. The mechanism of action is the same. The therapeutic outcome, when the product meets quality standards, is the same.
Myth 6: Generic Medicines Are Expiry Medicine
Fact: A generic medicine is one whose patent has expired — not one whose shelf life has passed. Those two things are not the same thing!
When a pharmaceutical company develops a new drug, it is granted a patent that generally lasts for 20 years from the filing date. During this time, no one else can produce or market that drug except the patent holder. After the patent runs out, other manufacturers may market the same drug — with the same active ingredient, strength and dosage form — once they show bioequivalence. The US FDA states that the brand product must have been exclusively available for its patent period and only after a rigorous review are generic drugs approved (“Generic Drugs: Questions & Answers” — US FDA).
An expired medicine is, however, a medicine that has simply outlived its date of processing in addition to its specific shelf life. You can recognize it by looking at the expiry date or best-before date printed on the label. An expired medicine — be it branded or generic — should never be consumed, because its chemical stability may have diminished.
Paracetamol is a good example. Its patent expired years ago. Every single paracetamol tablet you pick up and pay for today — whatever Crocin or Dolo or Jan Aushadhi label it bears — is a generic. The patent on paracetamol expired as far back as 2007, and dozens of generic forms came into the market ranging from ₹0.22 to ₹3.64 per 500mg tablet (see: “The concept of: Generic drugs and patented drugs vs. brand name drugs and non-proprietary (generic) name drugs” — Desai RJ et al., Frontiers in Pharmacology, 2013). All of those are made from scratch and have an active expiration date. But all of them are not “expired medicine.”
References
- “Substandard and Falsified Medical Products” — World Health Organization, 2017 – https://www.who.int/news-room/fact-sheets/detail/substandard-and-falsified-medical-products
- “Impact of Counterfeit Products on Indian Economy” — ASSOCHAM India, 2015
- “A comparative evaluation of price and quality of some branded versus branded–generic medicines of the same manufacturer in India” — Singal GL et al., Indian Journal of Pharmacology, 2011 – https://pmc.ncbi.nlm.nih.gov/articles/PMC3081449/
- “Generic Drugs: Questions & Answers” — US FDA – https://www.fda.gov/drugs/frequently-asked-questions-popular-topics/generic-drugs-questions-answers
- “Bioequivalence of generic drugs: a simple explanation for a US Food and Drug Administration requirement” — Andrade C, Journal of Clinical Psychiatry, 2015 – https://pubmed.ncbi.nlm.nih.gov/26132680/
- “Generic drugs – The Indian scenario” — Shetty YC et al., Journal of Postgraduate Medicine, 2019 – https://pmc.ncbi.nlm.nih.gov/articles/PMC6515776/
- “Improving access to medicines by popularising generics: a study of India’s People’s Medicine scheme in two districts of Maharashtra” — BMC Health Services Research, 2022 – https://link.springer.com/article/10.1186/s12913-022-08022-1
- “The discovery of insulin revisited: lessons for the modern era” — Hirsch IB et al., Journal of Clinical Investigation, 2021 – https://pmc.ncbi.nlm.nih.gov/articles/PMC7773348/
- “Scientist Sold Insulin Patent for $1, Saying ‘It Belongs to the World’?” — Snopes, 2024 – https://www.snopes.com/fact-check/insulin-patent-dollar/
- Fawad Khan diabetes interview — ARY News, 2023 – https://arynews.tv/fawad-khan-experience-of-diabetes-diagnosis/
- “Health economics and effectiveness analysis of generic anti-diabetic medication from Jan Aushadhi: An ambispective study in community pharmacy” — Journal of Diabetes & Metabolic Disorders, 2021 – https://www.sciencedirect.com/science/article/abs/pii/S2212877821003234
- “Why the Jan Aushadhi Scheme Has Lost Its Steam in India?” — Rajagopal D, Journal of Pharmacology and Pharmacotherapeutics, 2017 – https://pmc.ncbi.nlm.nih.gov/articles/PMC5642129/
- “A Cost Analysis of the Jan Aushadhi Scheme in India” — Annals of Tropical Medicine and Public Health, 2017 – https://pmc.ncbi.nlm.nih.gov/articles/PMC5417146/
- “Medicine affordability and access in India: lessons from generic–branded price variation under the Jan Aushadhi Scheme” — Frontiers in Public Health, 2025 – https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2025.1629835/full
- “The concept of: Generic drugs and patented drugs vs. brand name drugs and non-proprietary (generic) name drugs” — Desai RJ et al., Frontiers in Pharmacology, 2013 – https://pmc.ncbi.nlm.nih.gov/articles/PMC3770914/